Direct Personal Healthcare Spending and its Impact on Poverty in the Arab Countries
Many Arab countries suffer from the absence of a comprehensive health insurance system that covers the entire population. In the absence of such a system, many Arab households depend on direct personal healthcare spending in the event of sickness of any family member. Therefore, a significant number of the population in the Arab countries experiences the constant threat of an economic disorder in the event of sickness.
The health shock is more severe if it hits the head of the family, who is usually the family’s main source of income and of living. In fact, sickness does not only lead to an increase in the family’s spending due to the requirements of the treatment but also leads to the lack of ability to work and thus secure an income. Unfortunately, many Arab countries suffer from labor in the informal sector, reaching 67% in the non-oil producing Arab countries and 6% in the oil-producing countries [1], which does not provide for sick leaves or social or health insurance.
Some families living in extreme poverty might avoid visiting healthcare providers as they are unable to provide medical expenses or to adapt to them. The result: these families enter into a vicious circle of poverty and disease that is difficult to get out from.
Figure 1: Direct personal healthcare spending in the Arab countries for the year 2014
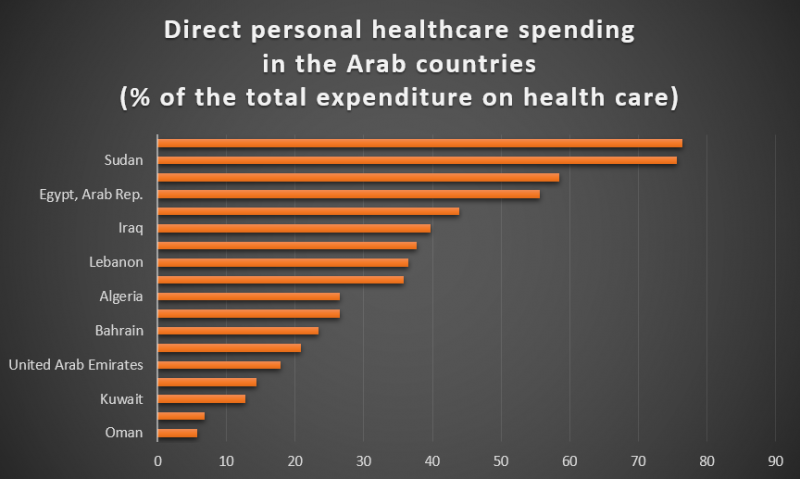
Source: World Bank database
Figure 1 illustrates the direct personal healthcare spending in the Arab countries for the year 2014 as a percentage of the total expenditure on healthcare; it appears that more than half of the healthcare expenditure in Egypt, Morocco, Sudan and Yemen was out-of-pocket expenses, and a third in each of Mauritania, Iraq, Tunisia, Lebanon and Djibouti. The figure also illustrates that Jordan, which is a middle-income country, was able to reduce the volume of direct personal healthcare spending reaching a level close to that in rich Arab countries. Despite the impact of these expenditures on the economic situation of families in the Arab countries and their contribution to their impoverishment, they are not taken into consideration in poverty estimates.
The problem with calculating poverty rates is that poverty lines do not distinguish between regular spending and indispensable healthcare spending.
Poverty estimates are based on a comparison of a household’s total spending against poverty lines; if the total expenditure, which may include medical expenses, exceeded the poverty line, the household is not considered to be poor. The problem with calculating poverty rates is that poverty lines do not distinguish between regular spending and indispensable healthcare spending. For instance, a family member might suffer from a chronic disease such as diabetes, the treatment of which requires periodic spending, and thus the household’s total spending might exceed the poverty line, thus it would not be considered poor, and accordingly cannot receive social benefits for example. However, this same family might be considered extremely poor after deducting healthcare expenses from its budget. When estimating the volume of poverty while taking healthcare expenditure into consideration in several Arab countries, we found that healthcare expenses are cause for increasing the percentage of poor people by approximately 3% in Egypt, 12% in Palestine, 4% in Lebanon, 1.6% in Yemen and 0.5% in Tunisia [2-4]. Current estimates of poverty in the Arab countries underestimate the real volume of poverty.
We are in need of new poverty estimates in the Arab region, ones that take into account the indispensable healthcare expenses, particularly in countries such as Egypt, Morocco, Sudan and Yemen, where direct personal healthcare spending poses a significant burden on the citizens. We also need to take quick steps toward implementing a system of comprehensive health insurance.
References
- Loayza, N. and T. Wada, Informal Labor in the Middle East and North Africa: Basic Measures and Determinants. Washington, DC: World Bank, 2010.
- Rashad, A. and M. Sharaf, Catastrophic Economic Consequences of Healthcare Payments: Effects on Poverty Estimates in Egypt, Jordan, and Palestine. Economies, 2015. 3(4): p. 216.
- Elgazzar, H., et al., Who Pays? Out-of-Pocket Health Spending and Equity Implications in the Middle East and North Africa. 2010.
- Mataria, A., et al., Catastrophic healthcare payments and impoverishment in the occupied Palestinian territory. Applied Health Economics and Health Policy, 2010. 8(6): p. 393-405.
Ahmed Rashad is a researcher in development economics, health economics, and applied econometrics. He holds a PhD in Economic Development and Socio-economic Inequalities in Health.
The views expressed here are solely those of the author in his/her private capacity and do not in any way represent the views of neither the Arab Development Portal nor the United Nations Development Programme.
